

- Frozen shoulder
- Painful stiff shoulder
- Periarthritis shoulder
- Adhesive Capsulitis
INTRODUCTION :
- Frozen shoulder causes pain and stiffness in the shoulder.
- Over time ,the shoulder becomes very hard to move
- After a period of worsening symptoms, Frozen shoulder tends to get better, although full recovery may take up to 3 years.
- Physical therapy, with a focus on shoulder flexibility, is the primary treatment recommendation for frozen shoulder

DEFINITION :
Frozen shoulder also known as Adhesive Capsulitis is an inflammatory condition characterized by painful restriction of both active and passive range of motion.
EPIDEMIOLOGY :
- It affects approximately 3% of the general population
- more common in women of 40-70 years old
- The incidence in patients with diabetes is reported to be 2 to 4 times higher than in the general population.
- Previous episodes of frozen shoulder on one side may cause its occurrence in contralateral side -12% chances
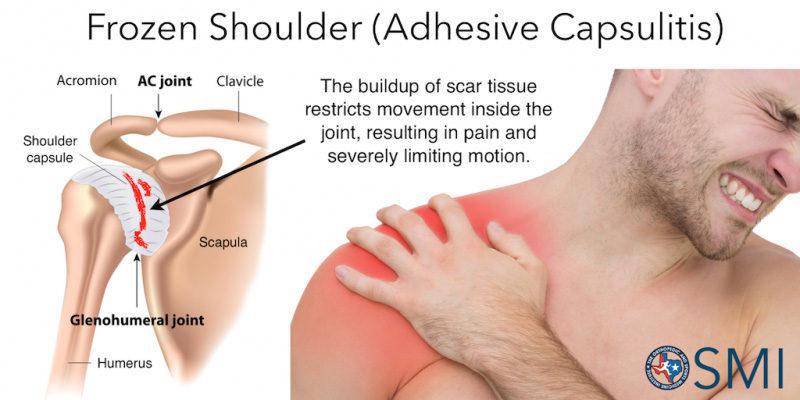
BASIC ANATOMY :
- The shoulder joint also known as GLENOHUMERAL JOINT is made up of three bones humerus (arm bone ) , the SCAPULA (shoulder blade) and the CLAVICLE (collar bone)
- This three bones joint together and held by ligaments , tendons
- All the ligament and tendon in shoulder joint are enclosed in a protective covering called CAPSULE within the joint
- CAPSULE consist of SYNOVIAL FLUID which lubricate the joint and helps in free movement
- Inflammation or injury in the Capsule leads to FROZEN SHOULDER

ETIOLOGY :
- The bones, ligaments and tendons that make up our shoulder joint is enclosed in a protective covering called CAPSULE. In frozen shoulder the shoulder capsule thickens and becomes stiff and tight. Thick bands of tissue called adhesion develop.
- In many cases, there is less synovial fluid in the joint.
- This thickened capsule gives less room for humerus head to move within the joint which restricts the movement.
- Movement may become stiff and painful

Risk factors :
Primary : onset is generally idiopathic
Secondary : Associated with some medical conditions
Shoulder cause : problems directly related to the shoulder joint which can give rise to frozen shoulder
- Rotator cuff tendinopathy (It cause tendons and muscles supporting shoulder joint to swell)
- Subacromial impingement syndrome (Inflammation of rotator cuff tendon as they pass through Subacromial space)
- biceps tendinopathy (Inflammation of the tendon around the long head of the biceps)
- Broken arm
- Fracture
- Dislocations
Non shoulder cause :Problems not related to shoulder joint
- Diabetes - 10 to 20% of people with diabetes develops frozen shoulder
- Post stroke
- Post operative
- Complication of Colles fracture (Fracture of distal radius)
- Reflex sympathetic dystrophy (lasting Pain in arm or leg after injury , stroke or heart attack)
- Hyperthyroidism
- Hypothyroidism
- Cardiovascular disease (cause referred pain in shoulder)
- Tuberculosis
- Parkinson's disease
PATHOPHYSIOLOGY :
- When one have hormonal imbalance or a weakened immune system, he or she may prone to joint inflammation like Frozen shoulder
- A long period of inactivity due to an injury , illness, or surgery also makes the joint stiff , vulnerable to inflammation and adhesion { bands of stiff tissue }.In serious case scar tissue (area of fibrous tissue that replaces normal tissue after an injury )may form.
- Immobilization of joint due to referred pain to shoulder like in Cardiovascular disease can lead to Frozen shoulder
- During abduction and repeated overhead activities of the shoulder,the long head of the biceps and the rotator cuff undergo repeated strain.This result in inflammation, fibrosis and consequent thickening of the capsule and finally there will be a loss of movement
PATHOLOGY :
- Inflammatory process causing Fibroblastic proliferation of joint capsule leading to thickening, fibrosis and adherence of the capsule to itself and humerus.
- leads to mechanical block to motions

CLINICAL PRESENTATION :
- Decreased range of both active and passive movement
- Pain is noted at the end stage of stretch
- Accessory joint play is reduced (rolling,gliding)
- Resistive tests are pain free in the available range of motion
- Patient unable to do the ADL (Activities of Daily Living) like combing hair, doing overhead activities
- Pain and restriction of motion depends on the stage of the disease
NOTE : Pain in Frozen shoulder does not radiate below elbow
Clinical Stages :
1.Freezing -
- Patients complains of acute pain
- decreased movement
- External rotation lost followed by abduction and forward flexion
- last for 10-36 weeks
2.Frozen -
- pain lessens but significant motion limitation affecting ADLs (Activities of Daily Living )
- last for 4-12 months
3.Thawing -
- pain is gone and motion improves but less than normal
- Last for 6 months to 2 years
DIFFERENTIAL DIAGNOSIS :
1.Acromioclavicular pathology :
- Eg; acromioclavicular joint injury, acromioclavicular arthritis
- pain may be present with weakness and stiffness related to pain
2.Subacromial impingement syndrome :
- Eg; rotator cuff tendinopathy, subacromial bursitis
- may present with preserved passive movement and history of repetitive overuse
3.Muscular tear :
- Eg; rotator cuff tear, long head of biceps tear)
- weakness often persist when shoulder pain is relieved
4.Autoimmune disease :
- Eg; Polymyalgia rheumatica, rheumatoid arthritis, systemic lupus erythematous
- may present with a polyarthropathy (five or more joints are affected) and systematic symptoms
DIAGNOSIS :
Physical examination
1.External rotation :
- External rotation in 0 position and compare it to other side
- External rotation loss of 50% compared to other side or less than 30 degree - positive
2.ROM reduction :
- ROM Should be reduced to atleast 25% in other two planes comparing to contralateral sides.
- check for full ROM for Adduction and flexion by fixating scapula and clavicle
Findings on physical examination :
- there may be loss of arm swing
- atrophy of deltoid muscle
- Generalized tenderness on palpations
- ROM (Range of motion) - limited range of motion, principally affecting external rotation and flexion of the shoulder joint
- Loss of full passive and active ROM
- pain at end of movements in all directions
3.Special tests :
Shoulder shrug sign -
Inability to lift the arm to 90 degree without elevating the whole scapula

Function related testing :

1.Hand to neck -A
- Shoulder flexion + abduction + External rotation
- Similar to ADLs such as combing hair,putting on a necklace
2.Hand to scapula -B
- Shoulder extension + adduction + Internal rotation
- Similar to ADLs such fitting a bra, putting on a jackpacket
3.Hand to opposite scapula -C
- shoulder flexion + horizontal adduction
- (The Scarf test - cross body adduction)
These tests requires appropriate elbow, scapulothoracic and thoracic mobility.If the patient unable to complete this motion other structures outside the shoulder joint may be the limiting factors.
X-ray ,MRI or CT is used to find out other etiology.
1. MRI -
- can reveal thickening of glenohumeral capsule
- to rule out tear in the rotator cuff
- loss of axillary recess indicates contracture of the capsule

2. X-ray - to check for arthritis

3. Injection test -
- Anesthetic injection is injected in the shoulder to numb the pain
- so that the doctor can better judge the active and passive range of motion.
TREATMENT :
- Frozen shoulder generally gets better over time although it may take up to 3 years.
- The focus of treatment is to control pain and restore motion and strength through physical therapy
1. NSAIDS :
Non steroidal anti inflammatory drug- can be used to reduce pain and swelling eg: aspirin,ibuprofen
2. Steroid injection :
Cortisone is a powerful anti-inflammatory medicine that is injected directly into the shoulder joint
3.Hydrodilatation :
- This procedure involves gently injecting a large volume of sterile fluid into the shoulder joint to expand and stretch the shoulder joint capsule .
- Hydrodilatation is conducted by a radiologist who uses imaging to guide the placement of fluid
4. Physical therapy :
will use fallowing technique
- Heat therapy wax bath is applied on shoulder to reduce stiffness before stretching
- Manual therapy and stretching
- Glenohumeral joint (shoulder joint ) mobilization
- Range of motion exercise to restore motion

SURGICAL TREATMENT :
- Surgery for frozen shoulder is typically offered during "STAGE -2 FROZEN.
- The goal of the surgery is to stretch and release the stiffened joint capsule.
1.Manipulation under anesthesia :
This procedure is performed when patient sedated in anesthesia the surgeon will move the shoulder through the range of motion which cause the capsule or scar tissue to stretch or tear
2. Arthroscopic capsular release :
In this procedure a radio frequency probe is inserted into the shoulder.The probe uses Radio frequency waves to cut the tissue capsule that surrounds the shoulder joint , allowing the shoulder to move more freely
Related articles :





1 Comments
Thank you for this wonderful and also helpful article
ReplyDelete